


免疫检查点抑制剂(ICIs)彻底改变了癌症治疗领域;然而,尽管将 ICIs 与各种治疗方式联合使用,仍有相当一部分患者疗效不佳,另外,约 60% 的患者在接受 ICIs 治疗时会因获得性耐药(AR)而病情进展,AR原因是 T 细胞耗竭和抗原呈递通路突变【1-4】。放射治疗(RT)是癌症治疗中最常见的手段【5】,能诱导免疫原性癌细胞死亡,释放肿瘤新抗原,并在与 ICIs 联合使用时触发局部和全身抗肿瘤反应【6,7】。尽管在一线转移性疾病中使用 RT + ICI 联合疗法的试验显示出希望【8,9】,但在难治性环境中,尤其是在对 ICIs 耐药的患者中,结果却令人失望【10,11】例如,在连续治疗中,10 名患有不同癌症类型且对 ICIs(PD-1 或 PD-L1 ± CTLA-4)有记录反应的患者重新接受了 ICIs 治疗加靶向 RT【12】,仅有一名患者出现体外反应(ORR 10%)。尽管如此,对于治疗选择有限的患者来说,增强这些放疗免疫疗法组合的有效性仍是一个未满足的需求。活化的树突状细胞(DC)将肿瘤新抗原呈递给抗原特异性 T 细胞,从而触发 T 细胞介导的肿瘤细胞杀伤【13】。树突状细胞的成熟是树突状细胞活化、抗原呈递以及下游 T 细胞共刺激的必要前提【14】。树突状细胞的发现,获得了2011年诺贝尔奖,树突状细胞在肿瘤微环境(TME)中发挥关键作用,以维持抗肿瘤 T 细胞效应反应【15】。肿瘤相关三级淋巴组织中成熟树突状细胞的高密度与 Th1 和细胞毒性偏移和更好的总生存期(OS)相关【16】。因此,增强树突状细胞成熟,从而提高抗原呈递能力的药物可能会提高放射免疫治疗的效果。几种微管解聚剂(MDAs),如长春碱、秋水仙碱和多拉司他汀,具有不同程度诱导树突状细胞成熟的能力,其中普林布林是效力最强的药物之一【17】。
近日美国安德森癌症中心放射肿瘤学教授Stephen Lin团队在在Med杂志发表题为Plinabulin following radiation enhances dendritic cell maturation and checkpoint inhibitor retreatment of relapsed/refractory cancers研究文章。研究表明,普那布林(Plinabulin)联合放疗和免疫检查点抑制剂,在人体实验中,可促进树突状细胞(DC)成熟,并在多种癌症且先前免疫检查点抑制剂(ICI)治疗失败的患者中产生肿瘤疗效。该研究还发现了一种潜在生物标志物——基线GEF-H1免疫特征,有助于筛选患者并预测临床疗效。
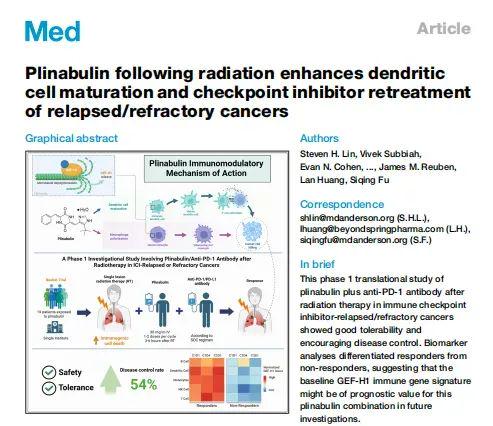
普那布林是新型(first-in-class)树突状细胞(DC)成熟促进剂,可逆性的结合于微管蛋白独特位点,解聚微管蛋白以释放 GEF-H1和促进经典单核细胞向炎症性 M1 型态转变【17-19】。免疫蛋白GEF-H1 激活 RhoA/ROCK 信号通路,促进 DC 成熟及抗肿瘤 T 细胞的免疫抗癌活性。该机制与传统微管蛋白作用药物不同,也不干扰紫杉烷类药物(如多西他赛)的抗癌活性。既往Dublin-3 三期临床研究表明:二/三线非小细胞肺癌,EGFR 野生型(n=559), 对照标准疗法多西他赛,普那布林 + 多西他赛显著延长总生存期,而且显著降低多西他赛的严重白细胞降低症【20】。303 二期临床研究表明:PD-1/L1进展的二/三线 非小细胞肺癌(n=47):普那布林 + 帕博利珠单抗 + 多西他赛联合治疗,中位无进展生存期(PFS)为 6.8 个月,15 个月总生存率(OS)达 78%【20】。本研究是在 诺贝尔奖得主 Ralph Steinman 博士和 Ira Mellman 博士奠定的树突状细胞激活免疫抗癌作用基础上的进一步探索【21】。
本研究为单臂、开放标签 I 期临床研究(NCT04902040),评估普那布林联合放疗与 PD-1 抑制剂在免疫检查点抑制剂治疗失败或复发患者中的安全性和抗癌疗效。主要终点为未照射病灶的客观缓解率(ORR,RECIST 1.1);次要终点包括疾病控制率(DCR)。治疗方案:放疗(第 1 周期及可选第 2 周期):局部整合放疗(8 Gy × 3 次;12.5 Gy × 4 次;或 4 Gy × 5 次),第 1 天开始;第 2 周期可选择性顺序放疗。普那布林:第 1 周期第 1 天及第 4 天(放疗后 3–6 小时)30 mg/m²;第 2 周期起每周期第 1 天;若第 2 周期进行放疗,第 4 天额外给药一次。PD-1 抑制剂:帕博利珠单抗每 21 天第 1 天 200 mg;或纳武利尤单抗每周期第 1 天 240 mg,每 14 天给药 2 次。
研究发现,抗癌临床结果:共有 19 名患者接受该联合方案,其中 14 人接受帕博利珠单抗(pembrolizumab),5 人接受纳武利尤单抗(nivolumab)。在 13 名 ICI 治疗失败患者中,客观缓解率(ORR)为 23%,疾病控制率(DCR)为 54%。并且在非小细胞肺癌 NSCLC(2/2)、头颈鳞状细胞癌HNSCC(2/3)和霍奇金淋巴瘤(2/2)患者中观察到临床获益(部分缓解或疾病稳定)。两名霍奇金淋巴瘤患者在 12及16 线既往治疗后仍获得超过 19 个月的持久缓解疗效。免疫作用机制确认:普那布林通过激活 GEF-H1 信号,在放疗后促进树突状细胞成熟。全血流式细胞术检测显示,DC 成熟标志物(CCR7、CD80、CD83)表达上调,并且应答者中单核细胞亚群由经典型向促炎型转变。
这些结果虽属早期,但提示普那布林通过树突状细胞成熟机制有望在逆转 ICI 获得性耐药方面发挥关键作用。尤其是在部分重度既往治疗患者中,我们观察到的长期疗效持续时间令人鼓舞,显示普那布林激活免疫系统的抗癌潜力。普那布林联合方案在非小细胞肺癌(NSCLC)、头颈鳞状细胞癌(HNSCC)和霍奇金淋巴瘤(HL)中取得了最佳疗效。生物标志物探索:单细胞 RNA 测序区分了应答者与非应答者,并发现基线 GEF-H1 免疫基因表达或可作为普那布林应答预测生物标志物。
综上所述,普那布林可促进树突状细胞成熟并激发免疫抗癌应答,为对检查点抑制剂治疗失败或复发的患者提供潜在的突破性治疗策略。
原文链接:https://www.cell.com/med/abstract/S2666-6340(25)00179-5
制版人:十一
参考文献
1.Badiyan, S.N., Roach, M.C., Chuong, M.D., Rice, S.R., Onyeuku, N.E., Remick, J., Chilukuri, S., Glass, E., Mohindra, P., and Simone, C.B., 2nd. (2018). Combining immunotherapy with radiation therapy in thoracic oncology.J.Thorac. Dis.10, S2492–S2507. https://doi.org/10.21037/ jtd.2018.05.73.
2. Meric-Bernstam, F., Larkin, J., Tabernero, J., and Bonini, C. (2021). Enhancing anti-tumour efficacy with immunotherapy combinations.Lancet397, 1010–1022. https://doi.org/10.1016/S0140-6736(20)32598-8.
3. Cai, Z., Zhan, P., Song, Y., Liu, H., and Lv, T. (2022). Safety and efficacy of retreatment with immune checkpoint inhibitors in non-small cell lung cancer: a systematic review and meta-analysis.Transl. Lung Cancer Res.11, 1555–1566. https://doi.org/10.21037/tlcr-22-140.
4. Memon, D., Schoenfeld, A.J., Ye, D., Fromm, G., Rizvi, H., Zhang, X., Keddar, M.R., Mathew, D., Yoo, K.J., Qiu, J., et al. (2024). Clinical and molecular features of acquired resistance to immunotherapy in non-small cell lung cancer.Cancer Cell42, 209–224.e9. https://doi.org/10.1016/j.ccell. 2023.12.013.
5. Baskar, R., Lee, K.A., Yeo, R., and Yeoh, K.W. (2012). Cancer and radiation therapy: current advances and future directions.Int. J. Med. Sci.9, 193–199. https://doi.org/10.7150/ijms.3635.
6. Herrera, F.G., Bourhis, J., and Coukos, G. (2017). Radiotherapy combination opportunities leveraging immunity for the next oncology practice.CA Cancer J. Clin.67, 65–85. https://doi.org/10.3322/caac.21358.
7. Golden, E.B., Marciscano, A.E., and Formenti, S.C. (2020). Radiation Therapy and the In Situ Vaccination Approach.Int. J.Radiat. Oncol. Biol. Phys.108, 891–898. https://doi.org/10.1016/j.ijrobp.2020.08.023.
8. Formenti, S.C., Rudqvist, N.P., Golden, E., Cooper, B., Wennerberg, E., Lhuillier, C., Vanpouille-Box, C., Friedman, K., Ferrari de Andrade, L., Wucherpfennig, K.W., et al. (2018). Radiotherapy induces responses of lung cancer to CTLA-4 blockade.Nat. Med.24, 1845–1851. https://doi.org/ 10.1038/s41591-018-0232-2.
9. Theelen, W.S.M.E., Chen, D., Verma, V., Hobbs, B.P., Peulen, H.M.U., Aerts, J.G.J.V., Bahce, I., Niemeijer, A.L.N., Chang, J.Y., de Groot, P.M., et al. (2021). Pembrolizumab with or without radiotherapy for metastatic non-small-cell lung cancer: a pooled analysis of two randomised trials.Lancet Respir. Med.9, 467–475. https://doi.org/10.1016/S2213-2600 (20)30391-X.
10. McBride, S., Sherman, E., Tsai, C.J., Baxi, S., Aghalar, J., Eng, J., Zhi, W.I., McFarland, D., Michel, L.S., Young, R., et al. (2021). Randomized Phase II Trial of Nivolumab With Stereotactic Body Radiotherapy Versus Nivolumab Alone in Metastatic Head and Neck Squamous Cell Carcinoma.J. Clin. Oncol.39, 30–37. https://doi.org/10.1200/JCO.20.00290.
11. Schoenfeld, J.D., Giobbie-Hurder, A., Ranasinghe, S., Kao, K.Z., Lako, A., Tsuji, J., Liu, Y., Brennick, R.C., Gentzler, R.D., Lee, C., et al. (2022). Durvalumab plus tremelimumab alone or in combination with low-dose or hypofractionated radiotherapy in metastatic non-small-cell lung cancer refractory to previous PD(L)-1 therapy: an open-label, multicentre, randomised, phase 2 trial.Lancet Oncol.23, 279–291. https://doi.org/10.1016/ S1470-2045(21)00658-6.
12. Chua, K.L.M., Fehlings, M., Yeo, E.L.L., Nardin, A., Sumatoh, H., Chu, P.L., Nei, W.L., Ong, E.H.W., Woo, W.Y., Low, K.P., et al. (2020). High-Dimensional Characterization of the Systemic Immune Landscape Informs on Synergism Between Radiation Therapy and Immune Checkpoint Blockade.Int. J.Radiat. Oncol. Biol. Phys.108, 70–80. https://doi.org/ 10.1016/j.ijrobp.2020.06.007.
13. Del Prete, A., Salvi, V., Soriani, A., Laffranchi, M., Sozio, F., Bosisio, D., and Sozzani, S. (2023). Dendritic cell subsets in cancer immunity and tumor antigen sensing.Cell. Mol. Immunol.20, 432–447. https://doi.org/10.1038/s41423-023-00990-6.
14. Mildner, A., and Jung, S. (2014). Development and function of dendritic cell subsets.Immunity40, 642–656. https://doi.org/10.1016/j.immuni.2014. 04.016.
15. Mellman, I., Chen, D.S., Powles, T., and Turley, S.J. (2023). The cancer-immunity cycle: Indication, genotype, and immunotype.Immunity56, 2188–2205. https://doi.org/10.1016/j.immuni.2023.09.011.
16. Goc, J., Germain, C., Vo-Bourgais, T.K.D., Lupo, A., Klein, C., Knockaert, S., de Chaisemartin, L., Ouakrim, H., Becht, E., Alifano, M., et al. (2014). Dendritic cells in tumor-associated tertiary lymphoid structures signal a Th1 cytotoxic immune contexture and license the positive prognostic value of infiltrating CD8+ T cells.Cancer Res.74, 705–715. https://doi. org/10.1158/0008-5472.CAN-13-1342.
17. Kashyap, A.S., Fernandez-Rodriguez, L., Zhao, Y., Monaco, G., Trefny, M. P., Yoshida, N., Martin, K., Sharma, A., Olieric, N., Shah, P., et al. (2019). GEF-H1 Signaling upon Microtubule Destabilization Is Required for Dendritic Cell Activation and Specific Anti-tumor Responses.Cell Rep.28, 3367–3380.e8. https://doi.org/10.1016/j.celrep.2019.08.057.
18. La Sala, G., Olieric, N., Sharma, A., Viti, F., de Asis Balaguer Perez, F., Huang, L., Tonra, J.R., Lloyd, G.K., Decherchi, S., Dı´az, J.F., et al. (2019). Structure, Thermodynamics, and Kinetics of Plinabulin Binding to Two Tubulin Isotypes.Chem5, 2969–2986.
19. Natoli, M., Herzig, P., Pishali Bejestani, E., Buchi, M., Ritschard, R., Lloyd, G.K., Mohanlal, R., Tonra, J.R., Huang, L., Heinzelmann, V., et al. (2021). Plinabulin, a Distinct Microtubule-Targeting Chemotherapy, Promotes M1-Like Macrophage Polarization and Anti-tumor Immunity.Front. Oncol.11, 644608. https://doi.org/10.3389/fonc.2021.644608.
20. Han, B., Feinstein, T., Shi, Y., Chen, G., Yao, Y., Hu, C., Shi, J., Feng, J., Wu, H., Cheng, Y., et al. (2024). Plinabulin plus docetaxel versus docetaxel in patients with non-small-cell lung cancer after disease progression on platinum-based regimen (DUBLIN-3): a phase 3, international, multicentre, single-blind, parallel group, randomised controlled trial.Lancet Respir. Med.12, 775–786. https://doi.org/10.1016/S2213-2600(24)00178-4.
21. R M Steinman, Z A Cohn. Identification of a novel cell type in peripheral lymphoid organs of mice. I. Morphology, quantitation, tissue distribution.J Exp Med., 1973, May 1;137(5):1142-62. doi: 10.1084/jem.137.5.1142.
(可上下滑动阅览)
BioArt
Med
Plants
人才招聘
学术合作组织
(*排名不分先后)

战略合作伙伴
(*排名不分先后)
转载须知
【非原创文章】本文著作权归文章作者所有,欢迎个人转发分享,未经作者的允许禁止转载,作者拥有所有法定权利,违者必究。


























热门跟贴